

Dr. Fauci’s Most Notable Critic
 “The PCR is a process. It does not tell you that you are sick.” –Dr. Kary Mullis, (image right) Nobel Laureate and Inventor of the RT-PCR, passed away in August 2019.
“The PCR is a process. It does not tell you that you are sick.” –Dr. Kary Mullis, (image right) Nobel Laureate and Inventor of the RT-PCR, passed away in August 2019.
“…All or a substantial part of these positives could be due to what’s called false positives tests.” –Dr. Michael Yeadon, distinguished scientist, former Vice President and Chief Science Officer of Pfizer
“This misuse of the RT-PCR technique is applied as a relentless and intentional strategy by some governments to justify excessive measures such as the violation of a large number of constitutional rights, … under the pretext of a pandemic based on a number of positive RT-PCR tests, and not on a real number of patients.” –Dr. Pascal Sacré, Belgian physician specialized in critical care and renowned public health analyst.
“I have seen massive efforts made to deliberately inflate Covid death numbers by relabelling cancer patients and stroke victims and all manner of normal regular deaths as Covid, in fact virtually anyone getting into an ambulance. The methods used to do so were totally flawed, PCR tests for example being run on 45 cycles we all know to be worthless, yet people are being euthanised on this basis and sometimes only on the basis of a chest x-ray alone.” –John O’Looney, Funeral Director, Milton Keynes, U.K.
From the outset of this crisis in January 2020, all far-reaching policy decisions upheld and presented to the public as a “means to saving lives” were based on flawed and invalid RT-PCR positive cases.
These invalid COVID-19 “estimates” have been used to justify confinement, social distancing, wearing of the face mask, the prohibition of social gatherings, cultural and sports events, the closure of economic activity, as well as the enforcement of the mRNA “vaccine” launched in November 2020. There is no such thing as a “COVID-19 confirmed case”.– Michel Chossudovsky, Professor of Economics (emeritus), University of Ottawa.
***
The late Dr. Kary Mullis, the inventor of the PCR test, has been blowing the whistle on Fauci and big pharma for 30 years.
Outstanding video production and analysis by Greg Reese
VIDEO. The Polymerase Chain Reaction Test
by Greg Reese
May the Late Dr. Kary Mullis’ Legacy Live.
*
The slanted methodology applied under WHO guidance for detecting the alleged spread of the virus is the Reverse Transcription Polymerase Chain Reaction (RT-PCR) test, which has been routinely applied all over the world since February 2020. (This Text below is an excerpt from Michel Chossudovsky’s book, August 2022)
The Reverse Transcription Polymerase
Chain Reaction (RT-PCR) test
by Michel Chossudovsky
The RT-PCR test has been used worldwide to generate millions of erroneous “COVID-19 confirmed cases”, which are then used to sustain the illusion that the alleged pandemic is real.
This assessment based on erroneous numbers has been used in the course of three and and a half years to spearhead and sustain the fear campaign.
“Confirmed” is a misnomer. A “confirmed RT-PCR positive case” does not imply a “COVID-19 confirmed case”.
“Positive RT-PCR is not synonymous with the COVID-19 disease! PCR specialists make it clear that a test must always be compared with the clinical record of the patient being tested, with the patient’s state of health to confirm its value [reliability]. (Dr. Pascal Sacré)
The procedure used by the national health authorities is to categorize all RT-PCR positive cases as “COVID-19 confirmed cases” (with or without a medical diagnosis). Ironically, this routine process of identifying “confirmed cases” is in derogation of the CDC’s own guidelines:
“Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms. The performance of this test has not been established for monitoring treatment of 2019-nCoV infection. This test cannot rule out diseases caused by other bacterial or viral pathogens.” (emphasis added)
The methodology used to detect and estimate the spread of the virus is flawed and invalid.
False Positives
The earlier debate at the outset of the crisis focused on the issue of “false positives.”
Acknowledged by the WHO and the CDC, the RT-PCR test was known to produce a high percentage of false positives. According to Dr. Pascal Sacré:
“Today, as authorities test more people, there are bound to be more positive RT-PCR tests. This does not mean that COVID-19 is coming back, or that the epidemic is moving in waves. There are more people being tested, that’s all.”
The debate on false positives (acknowledged by health authorities) points to so-called errors without necessarily questioning the overall validity of the RT-PCR test as a means to detecting the alleged spread of the SARS-CoV-2 virus.
The PCR Test Does Not Detect the Identity of the Virus
The RT-PCR test does not identify/detect the virus. What the PCR test identifies are genetic fragments of numerous viruses (including influenza viruses types A and B and coronaviruses which trigger common colds).
The results of the RT-PCR test cannot “confirm” whether an individual who undertakes the test is infected with SARS-CoV-2.
Failures of the PCR Test, Ridiculously Low Numbers
Even if the 2019 nCoV had been detected and duly identified, the numbers of PCR-RT confirmed (cumulative) positive cases in the period leading up to to March 11, 2020 used as a justification to enforce the Lockdown of more than 190 countries were ridiculously low. The 80,981 cases for China also pertains to confirmed (cumulative) PCR positive cases. Note the new cases in China (PCR positive) on March 12, 2020 are of the order of “321 new”

Image: Total cumulative cases on March 12, 2020 (Source: WHO)
For Further Details see:
By , December 10, 2023
 There Never Was a “New Corona Virus”, There Never Was a Pandemic,
There Never Was a “New Corona Virus”, There Never Was a Pandemic,
By Prof Michel Chossudovsky, November 03, 2024
The WHO on January 13, 2021, acknowledged that the PCR test was invalid. The official text of the WHO entitled “Nucleic Acid Testing (NAT) Technologies that Use Polymerase Chain Reaction (PCR) for Detection of SARS-CoV-2″ is featured in the Annex below.
The WHO’s Mea Culpa
by Michel Chossudovsky
WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology. (emphasis added)
WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.”
“Invalid Positives” is the Underlying Concept
This is not an issue of “Weak Positives” and “Risk of False Positive Increases”. What is at stake is a “Flawed Methodology” which leads to invalid estimates.
What this admission of the WHO confirms is that the estimate of covid positive from a PCR test (with an amplification threshold of 35 cycles or higher) is invalid. In which case, the WHO recommends retesting: “a new specimen should be taken and retested…”.
The WHO calls for “Retesting”, which is tantamount to “We Screwed Up”.
That recommendation is pro-forma. It won’t happen. Millions of people Worldwide have already been tested, starting in early February 2020. Nonetheless, we must conclude that unless retested, those estimates (according to the WHO) are invalid.
From the outset, the PCR test has routinely been applied at a Ct amplification threshold of 35 or higher, following the January 2020 recommendations of the WHO. What this means is that the PCR methodology as applied Worldwide has led to the compilation of faulty and misleading Covid statistics.
And these are the statistics which are used to measure the progression of the so-called “pandemic”. Above an amplification cycle of 35 or higher, the test will not detect fragments of the virus. Therefore, the official “covid numbers” are meaningless.
It follows that there is no scientific basis for confirming the existence of a pandemic.
Which in turn means that the lockdown / economic measures which have resulted in social panic, mass poverty and unemployment (allegedly to curtail the spread of the virus) have no justification whatsoever.
According to scientific opinion:
“if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the US), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97% (Pieter Borger, Bobby Rajesh Malhotra, Michael Yeadon, Clare Craig, Kevin McKernan, et al, Critique of Drosten Study)
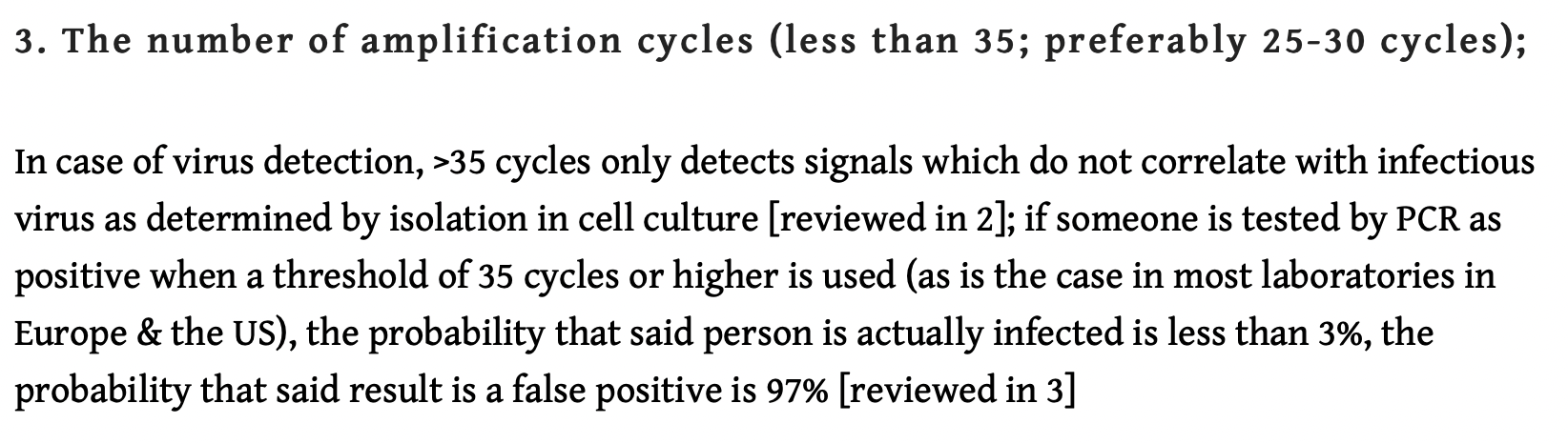
As outlined above, “the probability that said result is a false positive is 97%”: It follows that using the >35 cycles detection will indelibly contribute to “hiking up” the number of “fake positives”.
At the time of writing (mid-March 2021), despite the WHO retraction, the PCR test is being used extensively to hike up the numbers with a view to sustaining the fear campaign, justifying the ongoing lockdown policies as well as the implementation of the Covid vaccine.
Ironically, the flawed numbers based on “invalid positives” are in turn being manipulated to ensure an upward trend in so-called “Confirmed Covid -19 Cases”.
Moreover, those PCR tests are not routinely accompanied by a medical diagnosis of the patients who are being tested.
And now, national health authorities have issued (fake) warnings of a “Third Wave” as part of their propaganda campaign in support of the Covid-19 Vaccine.
The WHO confirms that the Covid PCR test procedure as applied is invalid. There is absolutely no scientific basis for implementing the Covid Vaccine.
Both the WHO and the scientific assessment of Pieter Borger, et al (quoted above) confirm unequivocally that the tests adopted by governments to justify the lockdown and the destabilization of national economies are INVALID.
Invalid Data and the Numbers’ Game
It should be understood that these “invalid estimates” are the “numbers” quoted relentlessly 24/7 by the media which have been used to feed the fear campaign and “justify” ALL the policies put forth by the governments:
- lockdown,
- closure of economic activity,
- poverty and mass unemployment,
- bankruptcies
- social distancing,
- face mask,
- curfew,
- the vaccine.
- the health passport
Invalid Data. Think Twice Before Getting Vaccinated
Michel Chossudovsky, November 9, 2024
For the complete text by the WHO dated, January 13, 2021 (Mea Culpa) see blow
Below is the WHO’s carefully formulated “Retraction”. (in Annex)
ANNEX
Nucleic Acid Testing (NAT) Technologies
that Use Polymerase Chain Reaction (PCR)
for Detection of SARS-CoV-2
Link to the original WHO Document
Product type: Nucleic acid testing (NAT) technologies that use polymerase chain reaction (PCR) for detection of SARS-CoV-2
Date: 13 January 2021
WHO-identifier: 2020/5, version 2
Target audience: laboratory professionals and users of IVDs.
Purpose of this notice: clarify information previously provided by WHO. This notice supersedes WHO Information Notice for In Vitro Diagnostic Medical Device (IVD) Users 2020/05 version 1, issued 14 December 2020.
Description of the problem: WHO requests users to follow the instructions for use (IFU) when interpreting results for specimens tested using PCR methodology.
Users of IVDs must read and follow the IFU carefully to determine if manual adjustment of the PCR positivity threshold is recommended by the manufacturer.
WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.
Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers must consider any result in combination with timing of sampling, specimen type, assay specifics, clinical observations, patient history, confirmed status of any contacts, and epidemiological information.
Actions to be taken by IVD users:
- Please read carefully the IFU in its entirety.
- Contact your local representative if there is any aspect of the IFU that is unclear to you.
- Check the IFU for each incoming consignment to detect any changes to the IFU.
- Provide the Ct value in the report to the requesting health care provider.
Notes
1. Diagnostic testing for SARS-CoV-2. Geneva: World Health Organization; 2020, WHO reference number WHO/2019-nCoV/laboratory/2020.6.
2. Altman DG, Bland JM. Diagnostic tests 2: Predictive values. BMJ. 1994 Jul 9;309(6947):102. doi: 10.1136/bmj.309.6947.102.
Click the share button below to email/forward this article to your friends and colleagues. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Birds Not Bombs: Let’s Fight for a World of Peace, Not War
Counter Information publish all articles following the Creative Commons rule creative commons. If you don't want your article to appear in this blog email me and I will remove it asap.

















No comments:
Post a Comment